
Peptide therapy sits between OTC supplements and full hormone replacement — more targeted than supplements, less heavy-handed than exogenous hormones. For men interested in optimization, this is the fastest-evolving category.
Growth Hormone Peptides
| Peptide | Mechanism | Administration | Best For |
|---|---|---|---|
| Sermorelin | GHRH analog — triggers natural GH pulse | SubQ injection, before bed | Natural-pattern GH elevation |
| Ipamorelin | Selective ghrelin receptor agonist | SubQ injection, 1-3x daily | Clean GH stimulation, minimal side effects |
| CJC-1295 (DAC) | Extended half-life GHRH analog | SubQ injection, 1-2x weekly | Sustained GH elevation, fewer injections |
| Tesamorelin | GHRH analog (FDA-approved for lipodystrophy) | SubQ injection, daily | Visceral fat reduction |
The Ipamorelin + CJC-1295 Stack
The most popular clinical protocol. Ipamorelin provides clean GH stimulation; CJC-1295 extends the release window. Together: synergistic GH elevation mimicking youthful pulsatility. Typical protocol: SubQ before bed, 5 days on / 2 days off. Expected effects over 3-6 months: improved sleep, faster recovery, reduced visceral fat, improved skin, increased lean mass.
Recovery Peptides
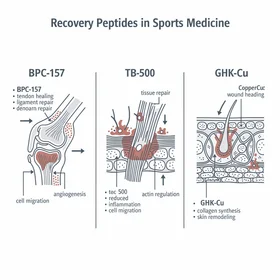
BPC-157 (Body Protection Compound)
Synthetic pentadecapeptide from gastric juice proteins. Extensive animal research showing accelerated healing of tendons, ligaments, muscle, bone, and gut tissue. Used by athletes for injury recovery. Available via SubQ injection or oral capsule.
Popular applications: tendon/ligament injuries, muscle tears, gut healing (IBS, leaky gut), joint inflammation.
Caveat: Almost all evidence is preclinical. Not FDA-approved. Available through compounding pharmacies.
TB-500 (Thymosin Beta-4)
Naturally occurring peptide involved in cell migration, angiogenesis, and tissue repair. Promotes new blood vessel formation, reduces inflammation, supports mobility in recovering joints. Often stacked with BPC-157 for comprehensive recovery.
Same regulatory caveat as BPC-157 — limited human data, not FDA-approved.
The Practical Progression
- Optimize lifestyle — sleep, training, nutrition (free, always step 1)
- Add OTC secretagogue — Sytropin for HGH support (~$60/mo, no prescription)
- Get bloodwork — baseline IGF-1 and testosterone levels
- Consider prescription peptides or TRT — if bloodwork shows clinical need and lifestyle optimization isn't sufficient
Don't skip to Tier 3 without doing Tiers 1 and 2. And never use prescription peptides without physician oversight.
Regulatory Landscape
The peptide space is evolving rapidly:
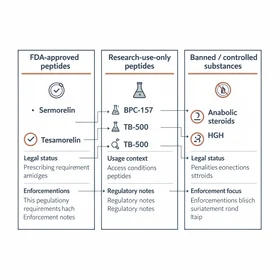
- Sermorelin, Ipamorelin, CJC-1295: Available through telemedicine men's health clinics. Legal when prescribed.
- BPC-157, TB-500: Not FDA-approved. Available through compounding pharmacies. FDA scrutiny increasing.
- The trend: More compounds being regulated, more compounding pharmacies being audited. Work with reputable providers who source quality-tested compounds.
Limitations & What to Know Before Starting Peptides
Peptide therapy is promising, but honesty about the limitations is essential for informed decision-making. Here's what the science actually supports -- and where the gaps are.
Limited Human Clinical Data
The most popular recovery peptides -- BPC-157 and TB-500 -- have impressive preclinical (animal) data but very limited published human clinical trials. Most human evidence is anecdotal or from clinical practice, not randomized controlled studies. Sermorelin and Ipamorelin have stronger human data, but even these lack the large-scale, long-term safety studies that drugs like testosterone have undergone (Sigalos & Pastuszak, Asian J Androl, 2018).
Side Effects & Safety Considerations
- GH peptides (Sermorelin, Ipamorelin, CJC-1295): Common side effects include water retention, tingling/numbness in extremities, increased hunger, and temporary blood sugar fluctuations. Rarely: headaches, joint stiffness, carpal tunnel-like symptoms. These typically resolve with dose adjustment.
- BPC-157: Generally well-tolerated in reported use, but long-term safety data in humans is absent. Theoretical concerns about promoting angiogenesis (new blood vessel growth) in individuals with existing tumors or cancer history. Caution is warranted.
- TB-500: Similar safety profile to BPC-157. May cause temporary lightheadedness, head rush, or lethargy at initiation. Same angiogenesis concern applies.
- Injection site reactions: Redness, swelling, or irritation at SubQ injection sites is common across all injectable peptides. Proper rotation technique minimizes this.
Regulatory & Quality Concerns
The peptide market has significant quality control variability. Compounding pharmacies are not held to the same manufacturing standards as FDA-approved drug facilities. Third-party testing (e.g., Certificate of Analysis from an independent lab) is the minimum standard you should demand from any provider. The FDA has increased enforcement actions against peptide sellers making therapeutic claims, and the regulatory landscape continues to tighten (FDA Warning Letters, 2024-2025).
Who Should Not Use Peptides Without Medical Clearance
- Anyone with a history of cancer -- the growth-promoting and angiogenic properties of GH peptides and recovery peptides require careful risk-benefit analysis with an oncologist
- Individuals with diabetes or insulin resistance -- GH elevation can affect blood sugar regulation; monitoring is essential
- Pregnant or nursing women -- no safety data exists for this population
- Anyone on blood thinners or with bleeding disorders -- some peptides may affect clotting pathways
The bottom line: peptide therapy has real potential, but it is not a casual supplement decision. Always consult a healthcare provider experienced in peptide protocols before starting. Get baseline bloodwork, use a reputable compounding pharmacy with third-party testing, and plan for ongoing monitoring. The science is advancing rapidly, but we are still in the early chapters of understanding long-term outcomes.